
Posted by Megan Van Noy on Nov 4 2024, 09:42 PM
Myofunctional therapy is a specialized treatment aimed at correcting orofacial myofunctional disorders (OMDs), addressing muscle dysfunction and improper oral habits. Myofunctional therapy (MT) has emerged as a critical intervention in pediatric dentistry, particularly in addressing sleep disordered breathing (SDB) and non-nutritive sucking habits (NNSH), and their impact on growth and development. This article reviews the role of myofunctional therapy in pediatric dentistry, focusing on its mechanisms, benefits, and the interdisciplinary approach required for optimal oral health and function in children.
The American Academy of Pediatric Dentistry (AAPD) defines the profession as an “age-defined specialty that provides both primary and comprehensive preventive and therapeutic oral health care for infants and children through adolescence.”Citation1 The focus on preventive care is customized to address the various stages and needs in oral health care, including monitoring growth and development in the pediatric population, early identification of sleep disordered breathing (SDB) and intervention of non-nutritive sucking habits (NNSH).
Myofunctional therapy (MT) is utilized to treat orofacial myofunctional disorders (OMDs), which are the disorders of the muscles and functions of the face and mouth. According to the Academy of Oral Myofunctional Therapy, “Orofacial Myofunctional Therapy is neurological re-education to assist the normalization of the developing, or developed, craniofacial structures and function. It is related to the study, research, prevention, evaluation, diagnosis, and treatment of functional and structural alterations in the region of the mouth (oro), face (facial), and regions of the neck (oropharyngeal area).” Myofunctional treatments are neuromuscular reeducation that optimizes muscle function and appropriate structural alignment in order to promote healthy growth and development. This is accomplished through targeted muscle exercises that improve tone, proprioception, and mobility.Citation2 Myofunctional therapy is a beneficial tool in several facets of pediatric dentistry including habit correction, interceptive treatment of sleep disordered breathing, and promotion of orofacial growth and development.
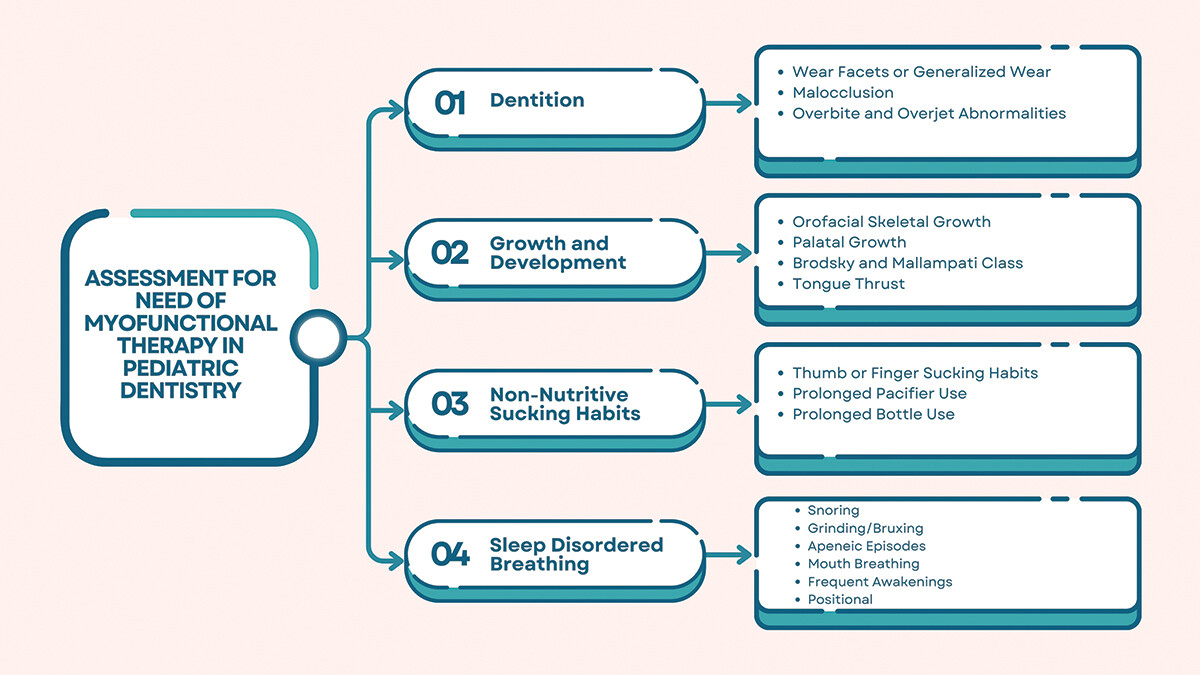
Identification of issues that can benefit from myofunctional therapy begins during intake. Identification will include NNSH, SDB, and overall growth and development deviations. Initial intake documentation can include current non-nutritive sucking habits such as finger sucking or pacifier use, sleep disordered breathing symptoms including snoring, grinding, apneic episodes or mouth breathing, orthodontic relationship and habits. Health history indicating muscular disorders or disorders with known craniofacial effects may indicate increased risk factors for needing intervention. Examination may further reveal clinically corroborating evidence such as wear facets, tongue thrust, palatal abnormalities, malocclusion, deep bite, anterior open bite, narrow airway, or tonsillar hypertrophy. Correlating these findings with the FAIREST-6Citation3 assessment or Pediatric Airway Assessment in the American Academy of Pediatric Dentistry Reference ManualCitation4 can provide a valuable screening tool for all patients. If risk factors are present, cotreatment with a myofunctional therapist may be indicated (Figure 1).
Figure 1. Process diagram of assessment for need of myofunctional in pediatric dentistry.
Sleep disordered breathing (SDB) describes not only obstructive sleep apnea, but also hypoxemia, upper airway resistance, hypoventilation, and central sleep apnea.Citation5 Symptoms associated with SDB include snoring, bruxing, open-mouth breathing, and periods of apnea. Frequently these symptoms are also associated with less restful sleep and have been related to daytime sleepiness and behavioral disorders.Citation2 The relationship between SDB and craniofacial features has not been well defined, but several studies point to an effect of breathing patterns on facial muscles, function, and efficacy of said muscles on upper airway resistance and frequency of collapse.Citation6 There is a strong correlation between snoring and adenotonsillar hypertrophy, as well as dentoskeletal anomalies such as underdevelopment of the maxillary arch and complicated occlusion patterns.Citation7 Tongue position, facial development, and oral habits play a strong role in the development of sleep disordered breathing issues.
The effects of myofunctional therapy on sleep disordered breathing symptoms have been well studied. Numerous peer-reviewed, evidence-based research articles show that breathing issues during sleep improved after six months of myofunctional therapy.Citation6 Myofunctional therapy focuses on strengthening the orofacial muscles, promoting nasal breathing, and improving the resting posture of the tongue. These interventions can reduce the severity of SDB by maintaining airway patency during sleep. Measures of Apnea-Hypopnea Indices (AHI) decreased in both pediatric and adult populations with myofunctional therapy, also improving snoring, oxygen saturation, and reports of sleepiness.Citation8 Adjunctive therapy with MT is effective for helping treat SDB while promoting continued healthy sleep habits.
Some studies show that non-nutritive sucking habits occur in up to 68% of children. Anterior open bite is associated with up to 38% of this population.Citation9 Prolonged NNSH (36 months or more) can lead to dental malocclusion, altered tongue posture, and orofacial dysfunction. These changes can predispose children to SDB and impact overall craniofacial growth and development.Citation10 Guilleminault et. al (2016) describe “the interaction between abnormal bone growth stimulation and the absence of nasal breathing with secondary development of mouth breathing is responsible for an abnormal development of the oral-facial bone structures supporting the upper airway, thus increasing the risk of upper airway collapse during sleep.”Citation11
Anterior open bite cause is multifactorial and is associated with non-nutritive habits, tongue thrust, open-mouth breathing, and genetic factors.Citation10 An anterior open bite leads to poor lip seal, which in turn can predispose one to mouth breathing. Tongue thrust is the persistence of infantile swallowing patterns past a developmentally appropriate time period.Citation2 Tongue thrust and anterior open bite are detrimental to continued growth. This pattern can cause speech difficulties, feeding difficulties, and temporomandibular joint disorders.Citation12
Myofunctional therapy is a critical tool in habit correction through neuromuscular reeducation and exercising of the oral facial muscles. These functional-based exercises target appropriate tongue posture and nasal breathing to activate the parasympathetic response via the maxillary palate and vagus nerve, thus eliminating the need for NNSH. After cessation of NNSH, anterior open bite can improve,Citation13 thus leading to improvements in craniofacial structure as the child continues development.
Facial development begins in utero during the eighth week of early embryogenesis when the palate is formed around the tongue and the tongue nearly fills the oronasal cavity.Citation14 Once the baby is born, the tongue continues to apply pressure to the palate, shaping it. Normal nasal breathing is typically observed when the tongue position is optimally high on the palate.Citation11 This position is the ideal position at birth, when normal activities can stimulate the intermaxillary synchondrosis, leading to natural palatal expansion and an ideal facial growth pattern.Citation11 The rest position of the tongue creates light forces which are key to morphogenetic development as the tongue in the functional matrix plays a plastic role due to its lack of neuromuscular spindles.Citation15 The role of the tongue in the stomatognathic system shapes the palate and is critical for proper bone growth.Citation16 A less than ideal tongue position can lead to decreased arch width, decreased airway growth, and increased detrimental cyclical breathing patterns. There are numerous contributing causes to a lowered position of the tongue, which can result in a high and/or narrow palate. One such correlating cause is mouth breathing, which has been demonstrated to jeopardize maxillofacial function and morphology.Citation17 Muscle weakness, tongue position, genetic predisposition for tongue space, and habits are additional contributing factors to facial growth and development.
The orofacial muscles play a crucial role in craniofacial development. Dysfunction in these muscles due to tongue position, SDB or NNSH can lead to abnormal growth patterns, including narrow dental arches and retrognathic mandibles. MT promotes normal muscle function, which can positively influence craniofacial growth and development. The literature in support of myofunctional therapy can be traced back to 1918 when Alfred Paul Rogers stated that this adjunct improved mandibular growth, nasal breathing, and facial appearance.Citation18 Early intervention with MT can help prevent or mitigate these developmental issues, leading to improved long-term outcomes for children.
Myofunctional therapy addresses several key areas in the pediatric dental population including orofacial muscle dysfunction and improper oral habits in children. Oral habits such as thumb sucking, tongue sucking, extended pacifier use, hair and clothing biting/sucking, tongue thrusting, and mouth breathing have been demonstrated to contribute to malocclusion, dental caries, and other dental issues.Citation2,Citation10,Citation12,Citation17 The correction of these habits through improved muscle function in the face, tongue, lips, and cheek muscles can encourage optimal facial growth and development. By targeting these areas, myofunctional therapy aims to improve their strength, coordination, and function, which in turn will contribute to proper chewing, swallowing, and speech development.
In the pediatric population, myofunctional therapy is designed to prevent or minimize the development of dental or malocclusion issues, which can reduce the need for more invasive treatments in the future. Early intervention is key to prevention and to guiding growth as the jaw is 50% developed by age 6 and 90% by age 12.Citation19 Therapeutic interventions improve neuromuscular function, strengthen muscles, and improve orofacial muscular contraction and sensitivity.Citation6
Establishing an appropriate tongue position allows ideal growth and development outcomes. Repositioning of the tongue can improve nasal breathing and decrease the symptoms of sleep disordered breathing.Citation6 In addition, appropriate tongue position decreases the extent of maxillary constriction, which is critical for development of the maxillofacial complex and upper airway.Citation18
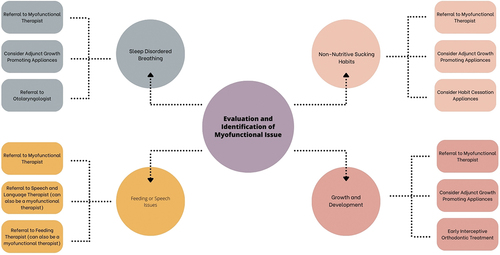
In recent years, the intersection of myofunctional therapy and pediatric dentistry has garnered significant attention for its role in addressing oral and facial muscle dysfunctions in children. Establishing a collaborative relationship between pediatric dentists and myofunctional therapists is crucial for early intervention and comprehensive treatment plans. To form this relationship, pediatric dentists should seek professionals who are certified by reputable organizations such as the International Association of Orofacial Myology (IAOM) or the Academy of Orofacial Myofunctional Therapy (AOMT). Networking at professional conferences, participating in interdisciplinary study groups, and utilizing professional directories are effective ways to locate qualified myofunctional therapists (Figure 2).
Figure 2. Evaluation and identification of myofunctional issues algorithm.
Myofunctional therapy is a highly collaborative field because it is function-based. In conjunction with pediatric dentists, orthodontists, speech-language pathologists, and other dental professionals, the team is able to provide comprehensive care for children with orofacial muscle dysfunction.
Myofunctional therapy offers a valuable tool in pediatric dentistry for addressing sleep disordered breathing and non-nutritive sucking habits and their impact on growth and development. By focusing on the function of the orofacial muscles through collaboration with a myofunctional therapist, MT can improve airway patency, promote healthy craniofacial growth, and aid in the cessation of detrimental habits. An interdisciplinary approach is essential for optimizing the benefits of MT and ensuring holistic care for pediatric patients.
There are no relevant financial or non-financial competing interests to report.
No potential conflict of interest was reported by the author(s).
Cherish K. Leung, DMD, MHA, MPH, FAAPD, maintains two private practices in Southern California. She is trained in oral myofunctional therapy through the International Association for Orofacial Myology. Dr. Leung is a fellow of the American Academy of Pediatric Dentistry.
Megan Van Noy, RDH, is a myofunctional therapist trained through the Academy of Orofacial Myology. She maintains a private practice in myofunctional therapy and leads several courses in the subject. In addition, she has a consulting business for implementing myofunctional therapy into a dental practice.
MON - FRI By appointments only.
SAT - SUN Closed


